Autoimmune Paranodopathies (Paranodal Neuropathies)
Definition:
Immune-mediated neuropathies targeting paranodal axo–glial junctions, distinct from CIDP, with different pathophysiology, clinical features, and treatment response.
🔹 1️⃣ Pathophysiology
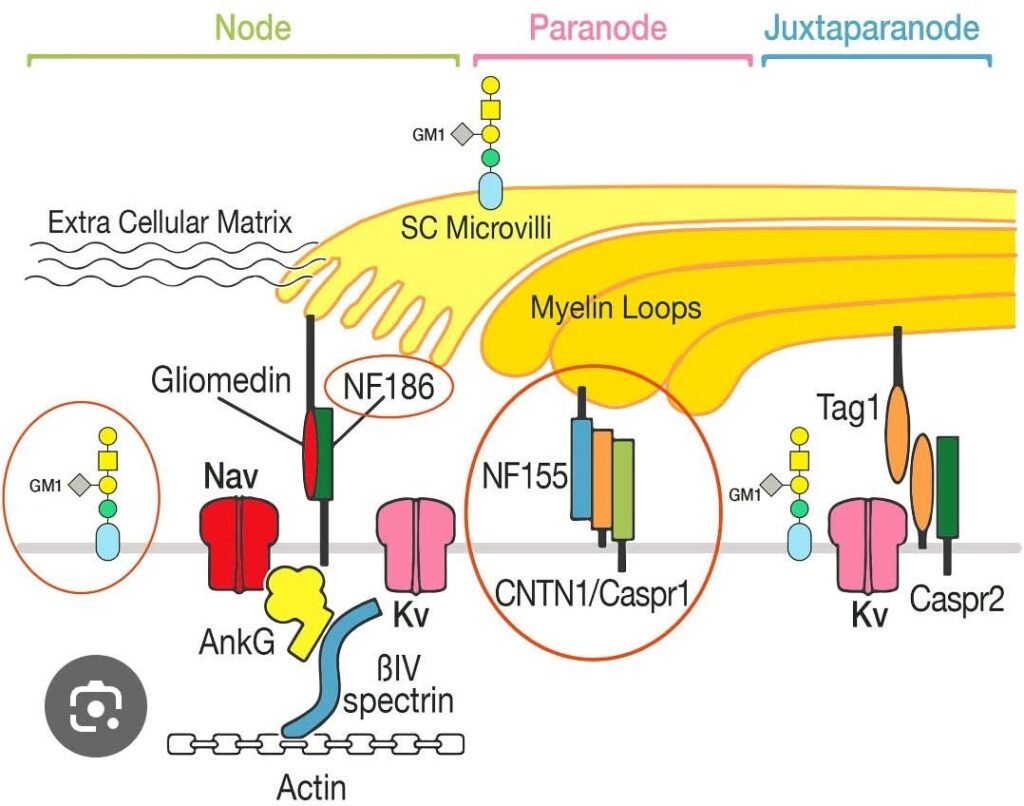
- 🧬 Target proteins at paranode:
- NF155 (glial)
- NF186 / NF140 (axonal)
- Contactin-1 (CNTN1)
- CASPR1
- ⚡ IgG4 antibodies:
- Minimal complement activation
- No macrophage-mediated demyelination
- 🧠 Effect: Node/paranode detaches → conduction failure without classic demyelination
🔹 2️⃣ Clinical Features
- Severe sensory ataxia (out of proportion to weakness)
- Prominent postural & kinetic tremor
- Early gait imbalance
- Subacute distal weakness or sensory loss
- Red flags for paranodopathy:
- Poor/no IVIG response
- Rapid progression
- Very high CSF protein
- Conduction block with minimal temporal dispersion
- Severe early symptoms
🔹 3️⃣ Antibody-Specific Phenotypes
| Antibody | Typical Patient | Features | Treatment Response |
|---|---|---|---|
| Anti-NF155 | Young (20–40) | Striking ataxia + tremor, distal weakness | Poor IVIG, ✅ Rituximab |
| Anti-CNTN1 | Older males | Motor-predominant, severe; nephropathy | Poor IVIG, ✅ Rituximab/PLEX |
| Anti-CASPR1 | Any | Pain prominent, may mimic acute CIDP | ✅ Rituximab/PLEX |
| Anti-NF186/NF140 | Any | More acute onset | Better IVIG response |
🔹 4️⃣ Electrophysiology
- Conduction block with minimal temporal dispersion
- Prolonged distal motor latencies
- Reduced CMAP amplitudes
- Myelin morphology preserved early
- ✅ Key distinction from classic CIDP
🔹 5️⃣ Diagnosis
- 🧪 Serum antibodies: NF155, NF186, CNTN1, CASPR1
- 💉 CSF: markedly elevated protein
- 🩻 MRI: possible nerve root thickening
- ⚕️ Kidney workup if CNTN1 positive
🔹 6️⃣ Treatment
Ineffective:
- ❌ IVIG (except NF186+)
Effective:
- 💉 Rituximab → first-line for IgG4 paranodopathies
- ⚗️ Plasma exchange (PLEX) → rapid improvement
- 🌡 Steroids: variable
Long-term:
- RTX every 6–12 months
- Consider azathioprine / mycophenolate as adjuncts
🔹 7️⃣ Prognosis
- ✅ Good if treated early before secondary axonal loss
- ❌ Poor if delayed diagnosis / IVIG-resistant
- Rituximab dramatically improves long-term outcomes
💡 High-Yield Clinical Pearl
- Severe sensory ataxia + tremor + conduction block with minimal temporal dispersion + NO IVIG response → excellent response to Rituximab